Written by Dr. Péter Czétány, MD, Consultant Urologist
Erectile dysfunction (ED) is defined as a persistent (or recurrent) inability to achieve or maintain an erection sufficient for satisfactory sexual intercourse, whether the difficulty lies in attaining the erection or in maintaining it.
Its prevalence increases with age: it affects 52% of men between 40 and 70 years, and it is estimated that approximately 320 million men worldwide are currently affected.
The underlying causes primarily include hypertension, diabetes mellitus, metabolic syndrome, ischemic heart disease, various hormonal disorders (such as testosterone deficiency and thyroid disease), psychiatric conditions (depression and anxiety disorders), and neurological diseases (spinal cord injury, stroke, Parkinson’s disease).
It is important to note that erectile dysfunction may be one of the first manifestations of otherwise asymptomatic cardiovascular disease, therefore in men over 40, cardiological evaluation is required even in the absence of cardiac symptoms.
Significant risk is also posed by lifestyle factors, including physical inactivity, smoking, drug use, and excessive alcohol consumption.
Erectile dysfunction may coexist with other urological diseases, such as benign prostatic hyperplasia (BPH) and chronic pelvic pain syndrome (CPPS) / chronic prostatitis, and these conditions can worsen each other’s symptoms.
It may also occur after radical surgery (prostatectomy, cystectomy) or radiotherapy performed for malignant urological diseases (such as prostate cancer or bladder cancer).
Diagnosis
The first step in diagnosis is a detailed medical history, which must cover:
- existing comorbidities
- regular medications
- lifestyle factors
- risk factors (e.g., alcohol, smoking)
- and other sexual symptoms (libido, orgasm, ejaculation)
If necessary, the partner may also be involved in taking the sexual history.
The presence or absence of morning erections is also an important piece of information.
For the objective assessment of sexual symptoms, questionnaires are very useful; the most widely used validated test is the Erection Quality Index (IIEF – International Index of Erectile Function).
In middle-aged and older men, an organic cause is usually found, whereas in younger men, psychological factors (e.g., relationship problems, anxiety) are often identified.
Physical Examination
The next essential step is a physical examination, including evaluation of the external genitalia.
The physician should also consider the patient’s overall appearance, including secondary sexual characteristics (e.g., body hair), obesity, etc.
Laboratory Testing
Essential laboratory tests include:
- glucose metabolism and lipid profile (fasting glucose, HbA1c, lipid levels)
- hormone tests, primarily serum testosterone (measured between 7–11 a.m. in a fasting state)
- and additional tests when indicated (e.g., prolactin, LH, TSH, PSA)
In selected cases, specialized tests may be required, such as:
- penile duplex Doppler ultrasound
- angiographic studies
- nocturnal penile tumescence and rigidity testing
Principles of Treatment
It is essential that patients receive professional medical care and consult an andrologist or urologist, rather than relying on the many often unverified dietary supplements and internet-sold medications, which may delay effective treatment and may even be harmful.
Treatment strategy must be individualized, based on test results and a detailed consultation, taking into account the patient’s preferences.
In cases of testosterone deficiency (hypogonadism), if the patient is no longer planning to have children, testosterone replacement therapy (injections or gel) is the appropriate treatment.
If a psychological component is suspected, sexual psychological counseling is recommended.
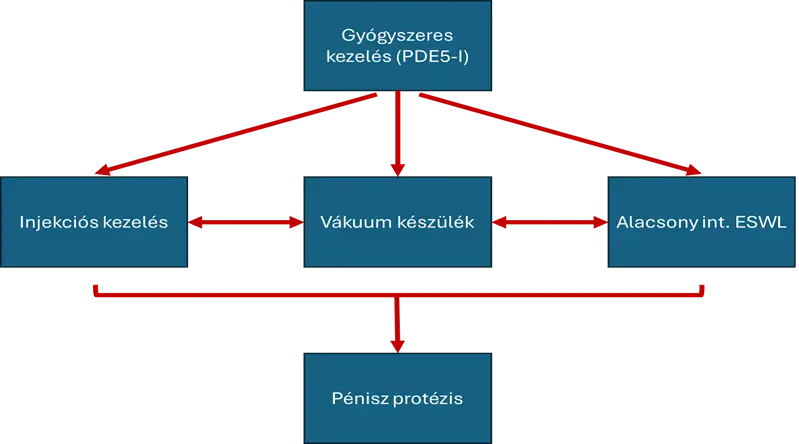
The treatment options shown at the top of the treatment chart are equally ranked, and patients may choose among them based on preference.
Low-intensity shockwave therapy (Li-ESWL) is only limitedly available in Hungary.
If first- and second-line treatments fail, penile prosthesis implantation becomes the final option.
Phosphodiesterase-5 Inhibitors (PDE-5 inhibitors)
These oral medications have revolutionized ED treatment since Viagra was introduced in 1997.
In Hungary, four agents are available: sildenafil, tadalafil, vardenafil, and avanafil.
They are highly effective and usually cause only mild side effects (headache, flushing, indigestion, nasal congestion, dizziness, back pain).
However, they must not be used in patients with:
- myocardial infarction within 3 months
- stroke within 6 months
- severe heart failure (≥ NYHA II)
- unstable angina
They also must not be combined with nitrate-containing medications due to the risk of severe blood pressure drop.
Sildenafil
The most commonly used “on-demand” drug.
Available in 25 mg, 50 mg, and 100 mg tablets.
Taken about 1 hour before intercourse.
Starting dose: 50 mg, adjusted based on effect.
Fatty meals reduce absorption.
Tadalafil
Known as the “weekend drug” due to its 24–36-hour duration.
Available in 5 mg, 10 mg, and 20 mg.
Taken at least 30 minutes before intercourse.
Starting dose: 10 mg.
Daily 5 mg dosing is considered when used at least twice weekly or when BPH/LUTS is present.
Vardenafil
Available in 5, 10, and 20 mg, also as an orally dissolving tablet, with faster onset.
Avanafil
Available in 50, 100, and 200 mg; the fastest-acting PDE-5 inhibitor, with effect within 20 minutes.
Intracavernosal Injection Therapy
A prostaglandin (PGE-1 analogue, alprostadil) is injected directly into the erectile tissue.
The dose is titrated, then self-administered by the patient.
Effect occurs in about 15 minutes.
Advantages:
- effective when PDE-5 inhibitors fail
- safe for high cardiovascular risk patients
Disadvantages:
- invasive
- injection pain, bruising
- rare priapism (erection lasting >4 hours)
- long-term fibrosis
Vacuum Device (Penis Pump)
A plastic cylinder creates a vacuum that draws blood into the penis; a silicone ring maintains the erection.
Useful in older men with multiple comorbidities who have infrequent sexual activity and cannot use other therapies.
Penile Prostheses
If all other options fail (e.g., in severe diabetes, vascular disease, spinal cord injury, post-cancer surgery), penile prosthesis implantation is the final option.
Two main types exist:
Semi-rigid prosthesis
Two rigid silicone rods implanted into the corpora cavernosa.
Advantages: simpler surgery, cheaper, fewer mechanical failures.
Disadvantage: penis remains permanently firm.
Hydraulic (inflatable) prosthesis
Consists of:
- two inflatable cylinders
- a pump
- a fluid reservoir
The pump in the scrotum transfers fluid to create erection and back to create flaccidity.
This most closely resembles a natural erection, but is more expensive and mechanically complex.
Sources:
Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994 Jan;151(1):54-61. doi: 10.1016/s0022-5347(17)34871-1.
Ayta IA, McKinlay JB, Krane RJ. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999 Jul;84(1):50-6. doi: 10.1046/j.1464-410x.1999.00142.x.
Saloni A, Bettocchi C, Capogrosso P, Carvalho J, Corona G, Dinkelman-Smit M, Hatzichristodoulou G, Jones TH, Kadioglu A, Martinez-Salamanca JI, Minhas S, Serefoglu EC, Verze P, Boeri L, Cocci A, Falcone M, Gül M, Kalkanli A, Morgado LA, Milenkovic U, Russo G, Bezuidenhout C, Smith EJ. EAU Guidelines on Sexual and Reproductive Health. (EAU Guidelines Office, Arnhem, The Netherlands, 2024).
Smith WB 2nd, McCaslin IR, Gokce A, Mandava SH, Trost L, Hellstrom WJ. PDE5 inhibitors: considerations for preference and long-term adherence. Int J Clin Pract. 2013 Aug;67(8):768-80. doi: 10.1111/ijcp.12074.
Az ábra felső részén egy sorban látható kezelési módozatok egymással egyenrangúak, azokat megismerve a páciens preferenciája alapján választhatunk közülük. Az alacsony intenzitású lökéshullám kezelés (Li-ESWL) hazánkban korlátozottan érhető el. Ezen, első- és második vonalban szereplő kezelések sikertelensége esetén jön szóba, utolsó lehetőségként a pénisz protézis implantációja. A következőkben ezen módszerekkel kapcsolatos lényegi tudnivalókat foglalom össze.
Foszfodiészteráz-gátlók (PDE5-I)
Az 5-ös típusú foszfodiészteráz-gátló (PDE5-I) hatóanyagok szájon keresztül szedhető gyógyszerformában alkalmazhatók, a Viagra 1997-es forgalomba hozatala óta forradalmasították az ED kezelését. Magyarországon jelenleg 4 hatóanyag van forgalomban: szildenafil, tadalafil, vardenafil, avanafil.
Ezen gyógyszerek igen jó hatékonyságúak, alapvetően kevés, enyhe mellékhatással (fejfájás, kipirulás, emésztési zavar, orrdugulás, szédülés, hátfájdalom, stb.) bírnak, azonban van néhány kórállapot, amikor nem alkalmazhatóak: 3 hónapon belül lezajlott szívinfarktus, 6 hónapon belül lezajlott sztrók, súlyos szívelégtelenség (≥NYHA II), instabil angina. Ezeken túl a túlzott vérnyomás esés veszélye miatt nitrát tartalmú gyógyszerrel sem alkalmazhatók együttesen.
A szildenafil a leggyakrabban alkalmazott, ún. „on-demand” (alkalmankénti) szer. A piacon 25-,50-, illetve 100 mg-os kiszerelésben érhető el, kb. egy órával az aktus előtt szükséges alkalmazni. A javasolt kezdő dózis 50 mg, mely a hatás függvényében csökkenthető vagy növelhető, mindig a legkisebb hatásos dózis alkalmazandó. A gyógyszer felszívódását a zsíros ételek ronthatják.
A tadalafil az ún. „weekend-drug”, mivel rendkívül hosszú, akár 24-36 órás hatástartam is elérhető vele. Ez a szer 5-, 10-, illetve 20 mg-os kiszerelésben érhető el, legalább fél órával az aktus előtt szükséges bevenni, felszívódását az ételek kevésbé befolyásolják. A javasolt kezdő dózis 10 mg, amely a hatás függvényében csökkenthető vagy növelhető, szintén mindig a legkisebb hatásos dózis alkalmazandó. Amennyiben egy héten legalább két alkalommal alkalmazzák vagy a panaszok mellett prosztatamegnagyobbodás és vizelési zavarok (BPH/LUTS) is fennállnak, a napi adagolás (5 mg-os dózisban) megfontolandó.
A másik két, ritkábban alkalmazott hatóanyag közül a vardenafil (5, 10 ,20 mg) előnye, hogy szájban oldódó formulációban is elérhető és hatása gyorsabban épül fel, mint a korábban említett két szeré. Az avanafil (50, 100, 200 mg) a leggyorsabban ható PDE5 gátló, maximális hatékonyságát akár 20 perc alatt is elérheti.
Barlangos test injekciós kezelése
Alkalmazása során egy prosztaglandin nevű anyag (PGE1 analóg, alprosztadil) kerül injektálásra, követlenül a barlangos testbe. A hatásos dózist ki kell titrálni. Ezt követően a páciens már önállóan alkalmazhatja. Az injekciót a pénisz testének oldalsó területén szükséges beadni, annak fertőtlenítését követően, az orvosi útmutatásnak megfelelően. A hatás általában 15 perc alatt kialakul. A kezelés előnye, hogy PDE5 gátlók hatástalansága esetében is hatékony lehet, illetve, hogy magas szív-érrendszeri rizikójú betegek esetében is biztonságos. Hátránya a nagyobb invazivitás, melytől a betegek idegenkedhetnek, mellékhatása a beadás helyét érintő fájdalom, bevérzés, ritkán priapizmus (4 órán túl tartósan fennálló merevedés), hosszútávon fibrózis lehet.
Vákuum eszköz
Más néven „péniszpumpa”, mely egy műanyag harangból és egy szilikon gyűrűből áll. A műanyag hengerben vákuum hozható létre a levegő kipumpálásával, mely előidézi a barlangos testek vérbőségét, majd a szilikon gyűrűt a péniszgyökre csúsztatva az a merevedést fenntartja. Idős, sok társbetegséggel élő páciensek esetében lehet hasznos, akik csak alkalmanként élnek szexuális életet és a többi terápiás lehetőség azok kontraindikációja (PDE5-I) vagy kézügyesség hiánya (pl. injekció) nem jön szóba.
Pénisz protézisek
Amennyiben valamilyen okból egyik korábban említett alternatíva sem jelent megoldást a páciens számára (súlyos diabétesz/érbetegség, gerincevlő sérülés, korábbi onkológiai műtét (pl. radikális prosztatektómia), stb.), utolsó lehetőségként pénisz protézis beültetése jön szóba. Az itt használt protézisek hazánkban egyelőre sajnos csak magánegészségügy keretei között érhetők el.
Két alapvető típus létezik:
• Ún. szemirigid protézis
• Többrészes, ún. hidraulikus protézis
A szemirigid hímvessző protézis esetében 1-1 merevített szilikonrúd kerül behelyezésre a barlangos testekbe. Előnyös, hogy a műtét technikailag egyszerűbb, rövidebb, maga az implantátum olcsóbb, kevésbé hajlamos meghibásodásra, hátrányként a természeteshez kevésbé hasonlító merevedés említhető (a pénisz állandó merev állapotban van, kézzel egyenes helyzetbe hajlítva „aktiválható”).
A hidraulikus hímvessző protézisek általában három részből állnak:
- 2 db felfújható „henger” (cylinder)
- Pumpa
- Folyadéktartály (reservoir)
A barlangos testekbe kerülnek beültetésre a felfújható implantátumok, melyeket a pumpával irányítva a folyadéktartályban lévő folyadékkal feltöltve/azt a tartályba visszapumpálva tudunk merev/petyhüdt állapotba hozni. A pumpa diszkréten a herezacskóba, a folyadéktartály pedig a szeméremcsont felett a hasfal mögé/hasfalba kerül beültetésre.
A hidraulikus protézis által elért hatás közelíti legjobban a természetes erekciót, használata könnyedén elsajátítható, kényelmes megoldást jelent a betegek számára. Hátránya a magasabb költség, a komplexebb sebészi technika igénye, illetve az összetettebb, több alkatrészből álló rendszerre való tekintettel a magasabb meghibásodási arány.
Források:
Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994 Jan;151(1):54-61. doi: 10.1016/s0022-5347(17)34871-1.
Ayta IA, McKinlay JB, Krane RJ. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999 Jul;84(1):50-6. doi: 10.1046/j.1464-410x.1999.00142.x.
Saloni A, Bettocchi C, Capogrosso P, Carvalho J, Corona G, Dinkelman-Smit M, Hatzichristodoulou G, Jones TH, Kadioglu A, Martinez-Salamanca JI, Minhas S, Serefoglu EC, Verze P, Boeri L, Cocci A, Falcone M, Gül M, Kalkanli A, Morgado LA, Milenkovic U, Russo G, Bezuidenhout C, Smith EJ. EAU Guidelines on Sexual and Reproductive Health. (EAU Guidelines Office, Arnhem, The Netherlands, 2024).
Smith WB 2nd, McCaslin IR, Gokce A, Mandava SH, Trost L, Hellstrom WJ. PDE5 inhibitors: considerations for preference and long-term adherence. Int J Clin Pract. 2013 Aug;67(8):768-80. doi: 10.1111/ijcp.12074.